|
|
|||||||||||||||||||||||||||||||||||||
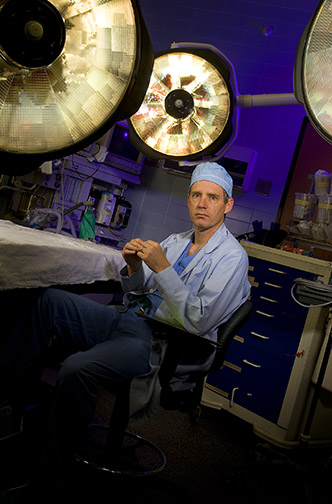
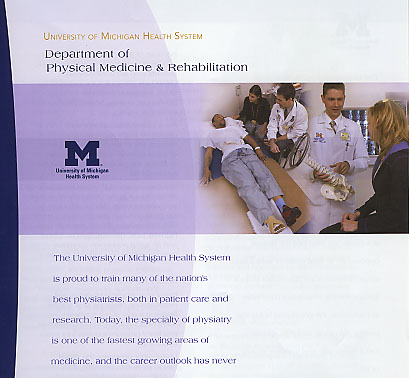
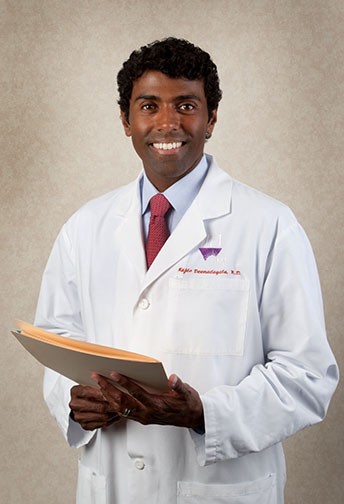
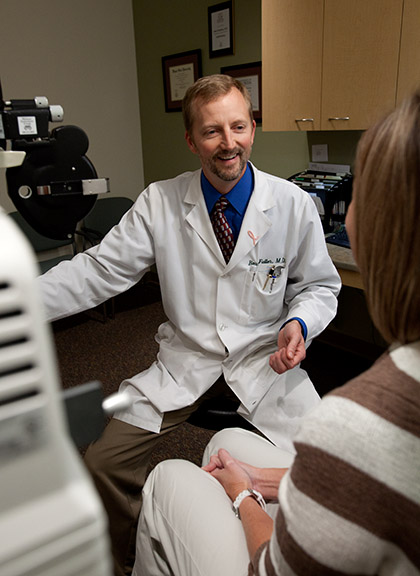
| Healthcare | |||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
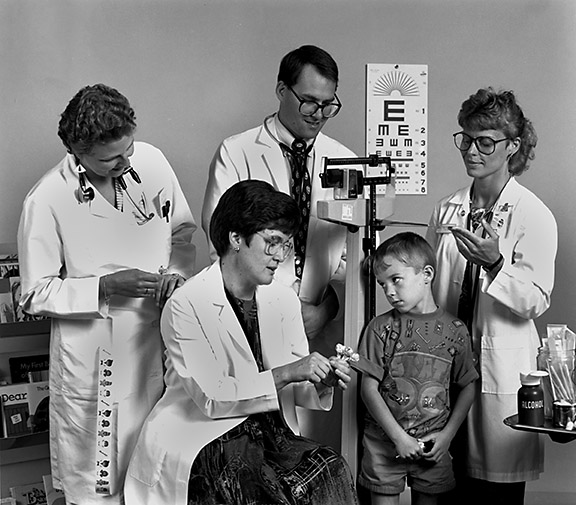
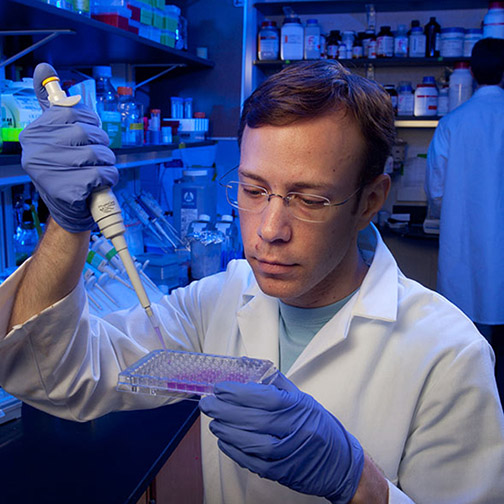
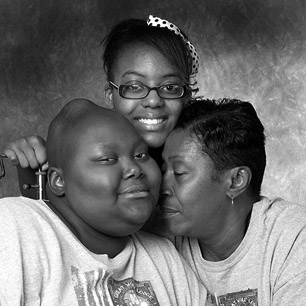
| Dwight has been providing medical photography to healthcare providers of all kinds since 1978. He brings a photojournalist's sensibilities to operating rooms and clinics to deliver strong images for recruiting brochures, annual reports, newsletters and displays. | |||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
 |
 |
||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||
 |
 |
 |
|||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
 |
 |
||||||||||||||||||||||||||||||||||||
 |
 |
 |
|||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
 |
 |
 |
|||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
 |
 |
||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
 |
 |
||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||
 |
 |
||||||||||||||||||||||||||||||||||||
 |
 |
 |
|||||||||||||||||||||||||||||||||||
| All photographs © Dwight Cendrowski | |||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||
| Dwight Cendrowski Ann Arbor Detroit medical Photographer | |||||||||||||||||||||||||||||||||||||